Nasal Sidewalls
The sidewalls of the nose influence how the central face transitions into the cheeks and under-eye area and can affect nearby fold patterns.
get started.webp)
The sidewalls of the nose influence how the central face transitions into the cheeks and under-eye area and can affect nearby fold patterns.
get startedThe nasal sidewalls are the lateral surfaces of the nose running from the nasal bridge to the alar base. The tissue here is thin and closely adherent to the underlying nasal cartilage, with limited subcutaneous fat. The adjacent anatomy — the nasolabial fold medially, the cheek fat compartments laterally — is what gives this area its clinical significance.
Treatment in the nasal sidewall region is almost always indirect: addressing cheek volume and the medial fat compartments that support the tissue adjacent to the nose, rather than injecting the nasal sidewalls directly. The fold that appears here is typically a consequence of midface descent rather than isolated nasal wall change.
The most common mistake in treating nasolabial folds is treating the symptom instead of the cause.
The nasal sidewalls are the lateral surfaces of the nose running from the nasal bridge to the alar base. The tissue here is thin and closely adherent to the underlying nasal cartilage, with limited subcutaneous fat. The adjacent anatomy — the nasolabial fold medially, the cheek fat compartments laterally — is what gives this area its clinical significance.
Treatment in the nasal sidewall region is almost always indirect: addressing cheek volume and the medial fat compartments that support the tissue adjacent to the nose, rather than injecting the nasal sidewalls directly. The fold that appears here is typically a consequence of midface descent rather than isolated nasal wall change.
The most common mistake in treating nasolabial folds is treating the symptom instead of the cause.
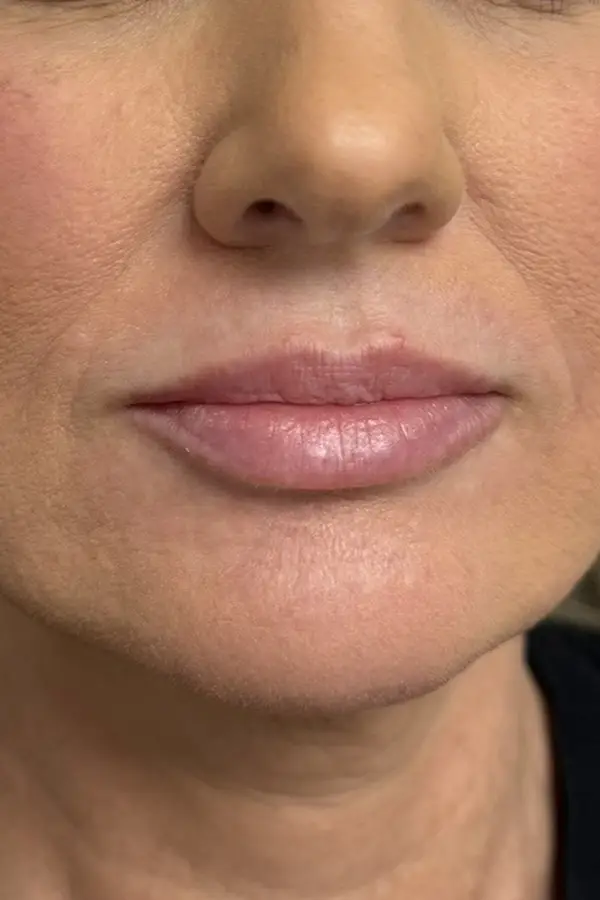
Nasolabial fold visible only with expression; tissue well-supported by full midface.
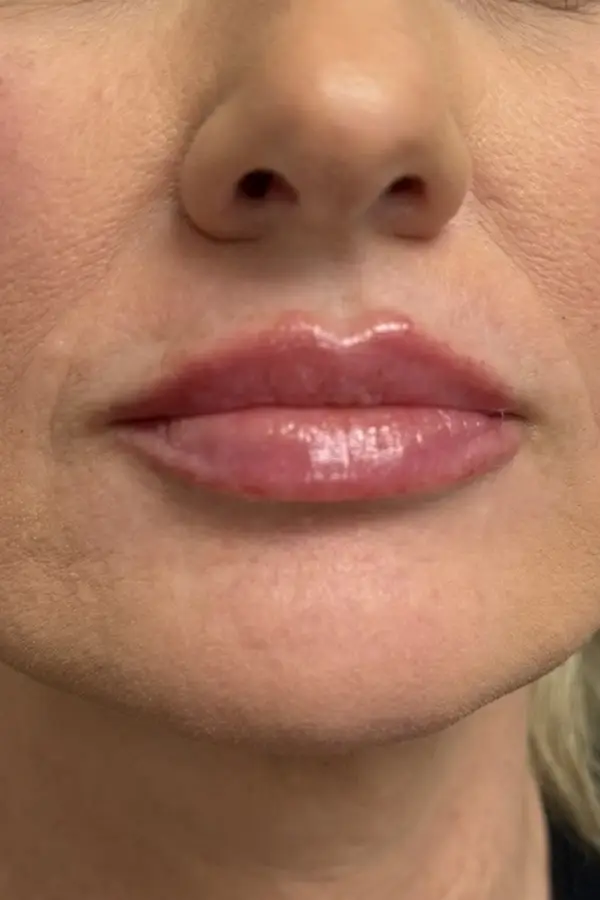
Early fold formation at rest as malar fat pad begins to descend.
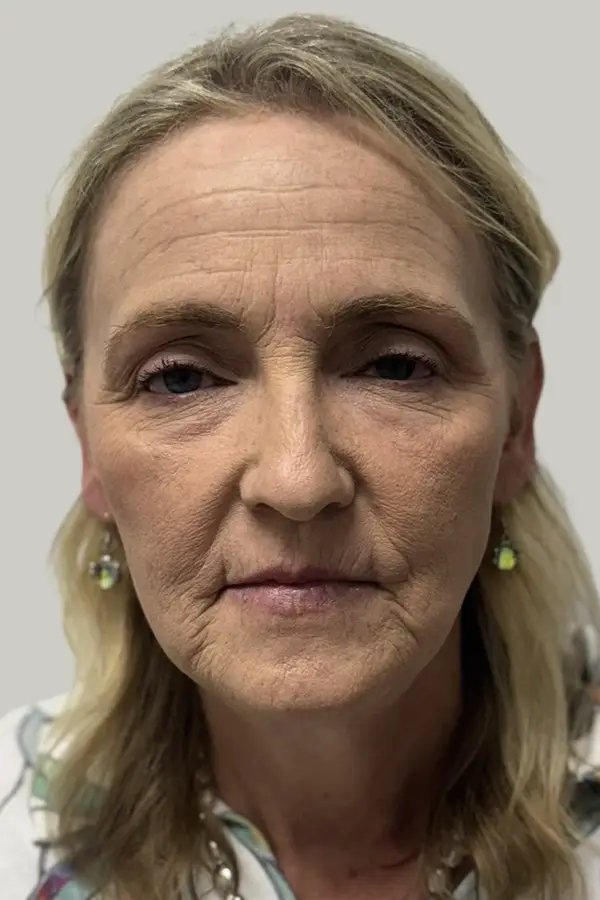
Established nasolabial fold at rest; midface descent accelerates fold depth.
Deep nasolabial fold with significant midface volume loss contributing to severity.
The tissue adjacent to the nasal sidewall is well-supported by the malar fat pad. Any nasolabial fold visible is dynamic — present only during expression.
Early malar descent allows the nasolabial fold to become faintly visible at rest. The nasal sidewall tissue begins to lose its supported, elevated quality.
Established fold at rest. Midface descent is the primary driver — the fold deepens as the tissue above it loses support.
Deep fold with significant midface deflation. The crease may have a structural component that requires both upstream support and direct softening.
Soften the nasolabial fold that runs from the nasal sidewall toward the mouth
Restore the midface support that's allowing the fold to deepen
Improve central face harmony without creating stiffness or unnatural volume
At CAMI, nasolabial fold treatment begins with assessment of the midface. A fold that exists primarily because the cheek has descended is best addressed by restoring cheek volume — which lifts the tissue that's creating the fold rather than just filling the crease. Treating the fold in isolation without addressing midface support produces a less natural result and requires more product.
When direct fold softening is appropriate, we use flexible filler products designed for dynamic areas to avoid stiffness on expression.

















































I'm blown away with my Dysport experience with Madison. She is very knowledgeable, professional and meticulous.
Meredith is the absolutely best!! She is so sweet and her work is perfection! Always an amazing experience at CAMI! Highly recommend.
.png)
I have been coming to CAMI for 5 to 6 years now and their service is bar none! I’m always exceptionally pleased with my results, as I rotate Botox and Xenomin. The staff are very friendly and I always make me feel right at home!
I can’t say enough about the entire team at CAMI and overall experience as a new patient. My concerns were addressed and at no point did I feel rushed or pressured to make a decision. Katie and the entire staff put me at ease. My results are amazing and have made me feel so much more confident. Thank you CAMI! Highly recommend!
.png)
Ashley at CAMI has been amazing. She made me feel comfortable before, during and after my treatments and helped me feel more confident in my appearance
I saw Madison for my Botox appointment and she was the best! She listened to my concerns and I’m very pleased with the results. She also recommended some great skincare products! Can’t recommend this office enough!
I had a wonderful experience with Madison Mikolajczyk,. From the very beginning, she explained everything about my face in detail and with such professionalism that I immediately felt comfortable. I truly appreciated her honesty in telling me exactly what I needed and what would work best for my features. She performed my filler injections using the cannula method and normal injections which left me with beautiful, natural-looking results—and no bruising at all. No one can do that using that method with no bruising. The entire process was completely painless, as she took her time and worked so gently.I couldn’t be happier with the outcome. My results are subtle, natural, and exactly what I hoped for. I’m truly in love with the way my face looks now and would highly recommend her to anyone seeking safe, professional, and natural enhancements. I did Sculptra, Botox and Radiesse filler looking forward for more.
I’ve had nothing but a great experience at CAMI! Ashley is amazing at what she does, as someone who has never gotten any kind of injections before, she was very knowledgeable explaining everything to you beforehand, and will make you feel as comfortable and confident as possible!
I have been very happy with my services over the past few months. Meredith is so sweet and always makes my time there very comfortable. She is patient with me and never pushes me into anything I’m not comfortable with regarding my skin.
I love visiting the CAMI location in Huntersville! They treat everyone special and I left feeling refreshed and uplifted. It was my first time meeting Katie, and she was spectacular! She spent time addressing my needs and concerns and I will definitely request an appointment with Katie again. Thank you CAMI!!
Very personable fun atmosphere and relaxing. Normally I go to California for my facials but I feel very good going to CAMI in Huntersville for my beauty needs.
Easy to schedule consult and treatments! Wonderful welcoming staff at CAMI who make you feel relaxed and excited to be there. Will continue to choose CAMI for all cosmetic needs and recommend to everyone!
This is a great place to come for any facial treatments, fillers, etc. The staff is excellent and I felt totally pampered.
The team is awesome. The staff takes great care of me. I would highly recommend CAMI.
The team was amazing. This was my 1st time getting Botox. They were very thorough and informative. They made the experience easy.
Their team is highly skilled and very good at what they do. I have never had any type of facial treatments before and decided it was time for a little pick-me-up. They took the time to listen to my concerns and recommended the procedure that was best suited for the outcome I was wanting.
Ashley is fantastic! Professional, friendly, and extremely knowledgeable. She’s my go-to for all my skincare maintenance needs. I always leave feeling confident and refreshed!
.png)
I was honestly skeptical about trying CAMI since I hadn’t had the best experiences with Botox and other treatments elsewhere. But choosing CAMI turned out to be one of the best decisions I’ve made. Madison, in particular, is the best nurse and injector I’ve ever worked with—she’s honest, genuinely cares about your results, and makes you feel like her top priority. While the treatments are an investment, as we age a little extra care and attention truly go a long way.
I Love CAMI, and all there staff! Katie Wilson is the absolute Beauty Making Queen!!! 👑 She is very particular when she was doing what I asked of and the results are perfection. I have recommended CAMI to multiple people and they are just as please. Thank you CAMI
I’m so glad I gave this med spa another chance. Everything feels completely different now in the best way. I had a hydrafacial and hydr with Meredith and noticed an immediate improvement in my skin. I went back and purchased a microneedling package, and the results have been good so far. Meredith truly made my experience there so much better. She made me feel comfortable, welcomed, and kept me laughing the entire time. She is also very honest, which I really appreciate. I’ve finally found my person, and I won’t let anyone else touch my face. Highly recommend!